
Recommended Articles

Will my children inherit my Grinch attitude at Christmas?
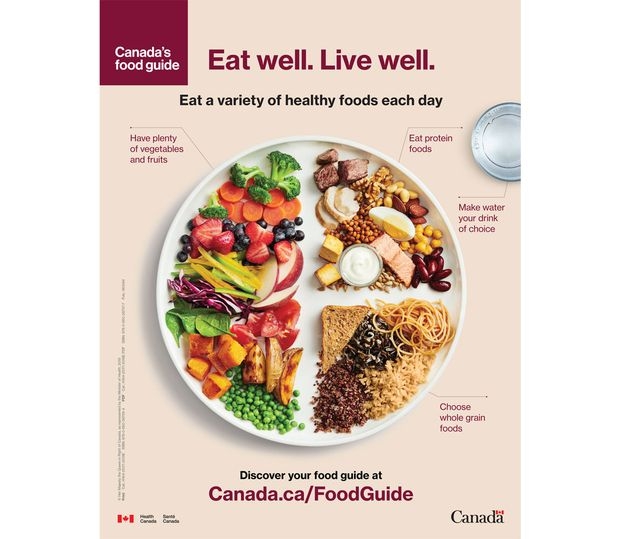
Two crucial next steps so the new Food Guide can really help Canadians eat better

Time to bring epilepsy awareness out of the dark ages





