
Recommended Articles
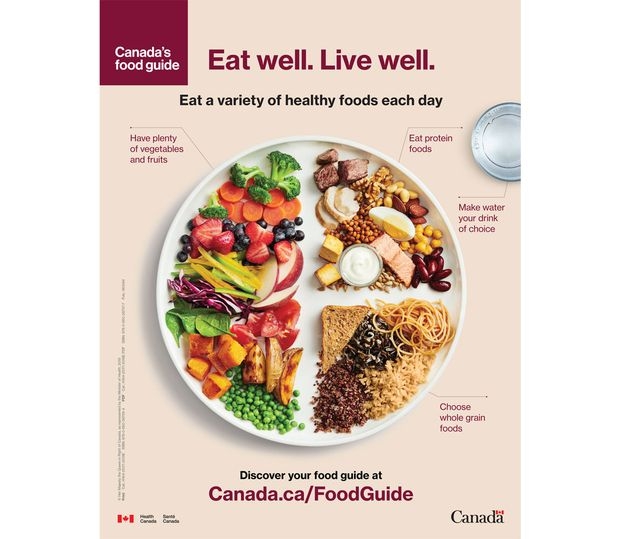
Two crucial next steps so the new Food Guide can really help Canadians eat better

An ever-aging population and its challenges for Canada’s health care system
Medically assisted dying cases need stronger review to safeguard us all






